What Is A Primary And Secondary Survey In Nursing?

The nursing sector, though holistic, is not homogenous. There are multiple departments, positions, and industries that students apply for. Nursing students learn about these concepts and theories as part of their curriculum. The modern-day nursing coursework includes vital subjects like patient care, trauma management, diagnosis and more.
Today, in this blog, I want to discuss a critical aspect of the nursing coursework that you must be familiar with. Here I want to outline a brief description and scope of the nursing survey. Now, there are two types of nursing surveys- primary and secondary
Both of these nursing survey categories are part of the trauma management course. The primary nursing survey is when the professional conduct a general study of the case when it is brought in. The secondary study delves deeper when the nursing staff tires a more advance approach to diagnosing the patient.
The nursing curriculum touches upon these survey types in detail. And if you have to write an assignment on the same, then this blog might be of some assistance. Here is all you need to know about the primary and secondary survey in nursing.
An excess of blood loss, increased pulse or erratic breathing can lead to sudden collapse or even death of the patient.
What is the primary study?
In the nursing sector, each medical case and patient is treated differently. And there are two ways or approaches to understanding a new situation. Now, trauma management and treatment are different from regular diagnosis. In trauma cases, the patient usually has some external force, psychological issues and more to deal with.
The primary survey, therefore, is a general approach wherein the student strives to understand the case from a generic perspective. This first general impression gives you an idea about the seriousness of the situation and how it affects the patient.
The primary survey also gives you an idea about the mental state and stress of the patient. Here, you check if the person is stable, conscious or has lost their senses.
Elements of the primary survey
There are six main steps to arrive at the primary study. This survey gives you a basic idea of the patient’s physical and mental status. It gives you an assessment of their body stats, pain levels and other such information.
Step 1: The general impression
The first step is to assess the state of the patient at a glance. You report this section as soon as the patient comes under your care. This helps you decide how serious the issue and how you want to tackle it.
The general first impression also helps the nurse decide the next best course of action. As a nursing student, you learn about the general approach to patient care with the primary survey report.
Step 2: Mental state
After checking the necessary condition of the patient, you need to understand how the patient is mentally affected. This refers not just to their emotional state but also the way they respond to or are conscious of their surroundings.
Mental awareness and stability also contribute to the patient’s diagnosis and the next course of treatment. The patient’s mental state is usually evaluated by the AVPU scale.

A- Alert: This refers to if the patient is awake, mentally alert and talking
V- Verbal: In some cases, the patient might be unresponsive at first but then respond to loud noise or stimulus
P- Painful: This refers to the patient’s senses and responds to pain. It also tells the nurse if the nervous system and muscles of the body are functional or not
U- Unresponsive: Here, the nurse tries to get a response from the patient with either verbal or pain stimuli (pressing against the breastbone for some reaction)
Step 3: Physical comfort
In case the patient has a history of mental or psychological issues, the diagnosis becomes more complicated. Here, the nurse usually contacts the caretaker or family of the patient for an underlying medical report.
Checking the physical comfort, position, and flexibility of the body comes next. This is where the nurse examines the body for any injuries and checks if the patient can move their limbs. The nurse also checks if the patient has any pain and swelling in any part of their body. They also check for external bleeding, cuts, bruises, abrasions, or rashes.
Step 4: Breathing issues and air passage
The fourth step is when the nurse checks for any blockages in the air passage. By this, I mean, the nurse examines if the patient can breathe properly. This is one of the most critical aspects of the diagnosis. The nurse can then decide the intensity of the case and take appropriate measures to help them breathe.
To facilitate breathing, you can stabilize the head and use the jaw-thrust movement method to open the air passage. The nurse also monitors the heartbeat, pulse and breathing rate of the patient. Sporadic breathing patterns are a concern, that can lead to chest congestions and eventual death.
Step 5: Circulation and Pulse
This is where the nurse checks for the pulse and blood circulation in the patient’s body. The vibration is usually found at the base of the neck or on the wrist. You can also place a hand on their chest to check for the heartbeat.
The body temperature, pressure, sugar levels and other stats are also recorded. Note that the nurse must be extra vigilant if the patient is old or has a history of heart-related issues.
Step 6: Look for injuries or bleeding
Note that the primary nursing survey is but a necessary report of the patient when they are first brought in. You don’t have to conduct an in-depth study of the case. However, if the patient is in the infant, a senior citizen or someone with serious medical history, then that must be taken into consideration.
An excess of blood loss, increased pulse or erratic breathing can lead to sudden collapse or even death of the patient.
What is the secondary survey?
The secondary survey comes after the primary study. This is where nurses delve deeper into the case and expand upon the findings of the initial report. The secondary review is also known as the focused history and physical examination process.
This is a more customized diagnosis, as opposed to the primary survey. For, while the fundamental review follows a standard approach, the secondary examination involves an in-depth analysis of the case. The secondary study supports a more focused approach to analyze the patient’s current state concerning their medical history.
Elements of the secondary survey
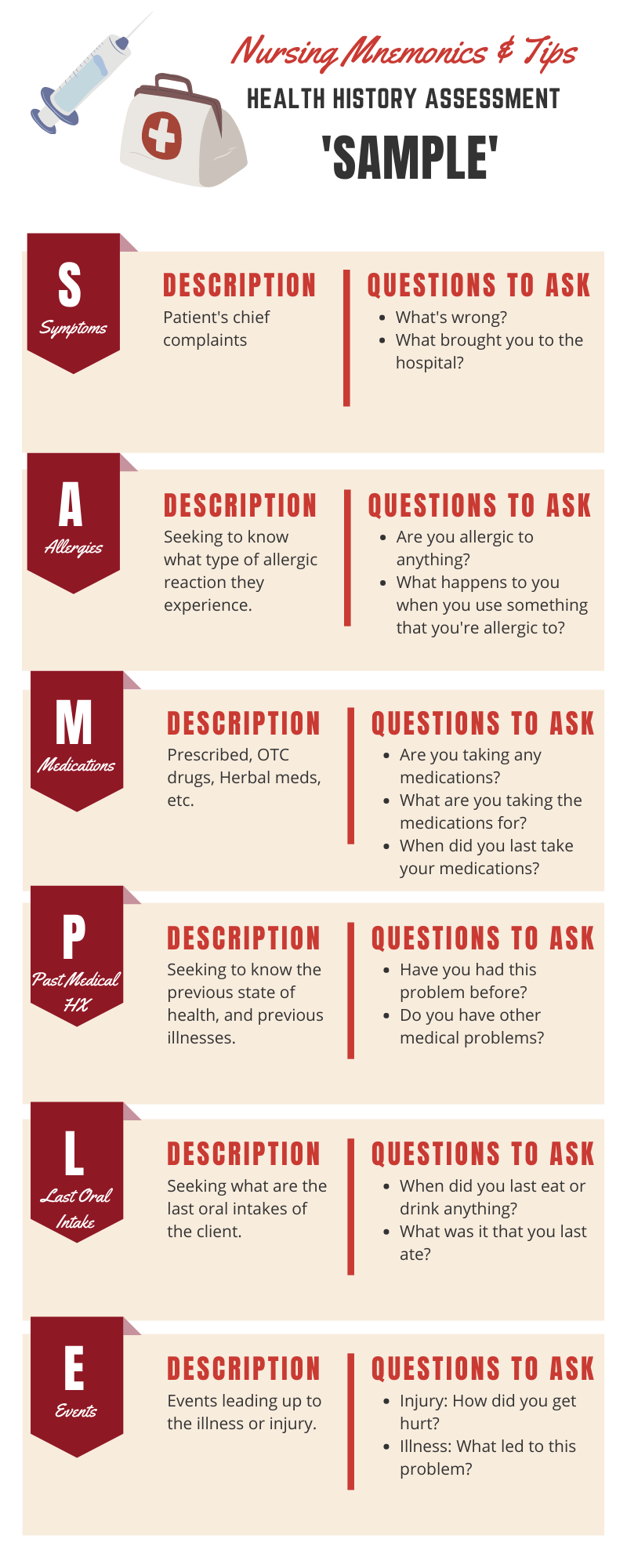
The secondary survey assumes that the patient is not under some immediate life-threatening concern. The initial treatment, injury check and breathing examination happen in the primary study. Here are some of the initial steps and elements required for secondary survey check-up. The acronym for this survey can be SAMPLE
S- signs and symptoms
A- allergies
M- medication
P- pertinent past medical history
L- last oral intake
E- events leading to the injury/illness
Each of these elements determines the cause of the patient’s present state. It also clarifies a lot of doubts for the doctor who can then prescribe the right treatment for the case.
Here, you also note the sudden changes in the patient’s physical or mental condition over the span between the primary and secondary survey taken.
How to write a nursing survey
The nursing survey begins with a short report on the patient as they enter the hospital premises and under your care. You first need to note their immediate physical condition and the most apparent signs you can see. Report all instances of injuries, blood loss and cuts on the body.
Then you check the breathing and another body state. The patient’s response to stimuli and pain is also noted down. Try to be as accurate in your description of the case as possible. All of this is part of the primary survey, where you indicate the first things you notice in the patient.
The secondary survey is where you go in-depth into the patient diagnosis. The first study is usually very generic and follows a standardized approach. The secondary examination is more personalized, where the nurse delves deeper into the patient’s medical history. It assumes that the immediate first aid has been given to the patient and that they are not under any fatal threat.
End the survey with a comparative study on how the patient’s health declines or improves throughout their treatment. A side by side study of the primary and secondary survey findings can give you a better idea about the patient’s progress.
Mental awareness and stability also contribute to the patient’s diagnosis and the next course of treatment.
Quick links and references
Primary Survey and Secondary Survey- US department of health and human services
Secondary survey emergency kit research paper
Nursing survey template and tools
The Bottom Line
The survey is an integral part of any nursing curriculum. It teaches you the basics of patient care and diagnosis. And the two categories of inquiries further simplify things for the nurses. It is easier to handle information when you section it in an orderly way.
I hope this blog was helpful for students to give them insights into nursing surveys.